
The healthcare environment is a known reservoir of multi drug resistant organisms (MDROs) and plays a significant role in the transmission of nosocomial pathogens and healthcare associated infections (HAIs)1. HAIs threaten patient safety and result in increased patient stay and increased costs to hospitals. A recent study estimated that, in one year in NHS general and teaching hospitals in England, there were 653,000 HCAIs which were estimated to account for a total of 5.6 million occupied hospital bed days and 62,500 days of absenteeism among front-line healthcare professionals2. This resulted in an estimated cost of £2.1 billion to the NHS in one year in England alone.
Environmental decontamination (through cleaning and disinfection) of the healthcare environment is a vital component to reduce the risk of transmission of HAIs and protecting patient safety. The National Infection Prevention and Control Manual (NCIPM) recommends the use of chlorine at 1,000 parts per million (ppm) for environmental decontamination under transmission-based precautions. Limitations of chlorine for disinfection include staff respiratory health challenges and equipment damage3. There is also the need to make up fresh solutions which poses a challenge in busy and time restricted environments, as well as challenges in ensuring the solutions are made to the required concentration4. Alternatives to chlorine include hydrogen peroxide, chlorine dioxide and peracetic acid which can be applied via wipes, sprays and mops (for bigger surface areas). Chlorine dioxide is a broad-spectrum oxidising agent, suitable for high-level disinfection of non-porous surfaces, including those of invasive and non-invasive medical devices5. Chlorine dioxide has a higher oxidation capacity, and a lower oxidation potential than most species of chlorine, making it more powerful per molecule. This characteristic allows chlorine dioxide to be effective at lower concentrations compared to other oxidising agents such as chlorine. Chlorine dioxide is compatible with surfactants and other chemicals which allow a solution with cleaning and disinfection abilities.
Within environmental decontamination there are numerous challenges posed by emerging and evolving microbial threats. These include Candidozyma auris, a fungal pathogen highly resistant to antimicrobial agents which can rapidly contaminate the healthcare environment6 and dry surface biofilms which have shown to persist in the environment for prolonged periods and withstand disinfection with chlorine7. Candidates for environmental decontamination should take into account emerging threats and ensure efficacy profiles are continually reviewed and updated. With this in mind as part of this study published in the Journal of Hospital Infection we evaluated chlorine dioxide against a panel of different MDROs and biofilms8.

In our study, solutions containing the active chlorine dioxide were evaluated against a panel of multidrug resistant bacteria including Methicillin resistant Staphylococcus aureus (MRSA) and Carbapenem resistant Enterobacterales (CRE), and C. auris using methods outlined in the European Norm (EN) 14885. As part of this study we evaluated different chlorine dioxide applications (including wipes, foams and liquids) with a concentration range of 120-200 ppm chlorine dioxide. All chlorine dioxide solutions produced a minimum of a 99.99% log reduction against the panel of microorganisms tested, meeting the criteria of the relevant standard tested to. Realistic and uniform contact times are vital for ensuring real word performance of disinfectants and all chlorine dioxide applications tested were effective at 5 minutes or less.

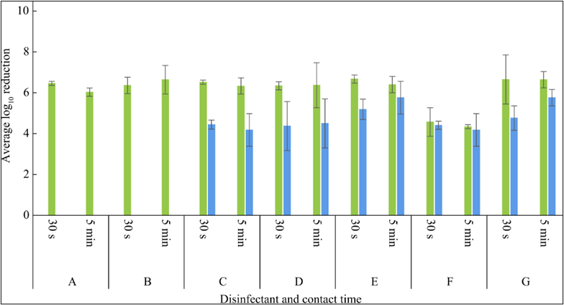
Given the role of biofilms in the contamination of the healthcare environment and the potential transmission of HAIs, we examined the performance of chlorine dioxide against biofilms formed by the commonly encountered Gram positive and Gram negative hospital pathogens Staphylococcus aureus and Pseudomonas aeruginosa, using the minimum biofilm eradication concentration assay (MBEC) (ASTM E2799). MBEC is used to evaluate the initial microbial kill of a disinfectant by introducing a biofilm to the test solution. All chlorine dioxide disinfectants tested against S. aureus and/or P. aeruginosa biofilms showed activity at both 30 second and 5-minute contact times (Figure 1). The disinfectants consistently achieved greater than 99.99% reductions against both organisms, with greater reductions shown against P. aeruginosa.
Figure 1 Efficacy of chlorine dioxide disinfectants against biofilms formed by Pseudomonas aeruginosa (green bars) and Staphylococcus aureus (blue bars).

Environmental decontamination of the healthcare environment plays an important role in protecting patient safety and therefore the choice of an appropriate and efficacious decontamination product is essential. A decontamination product should be broad spectrum in realistic contact times, safe to use (for staff and patients) and be easy to use and access (such as impregnated wipes or ready to use sprays). Given the challenges associated with transitional chlorine based disinfectants 3,4 and the need for decontamination products to keep pace with evolving threats (such as C. auris and biofilms), chlorine dioxide offers a viable alternative as highlighted in our study8.
1. Suleyman G, Alangaden G, Bardossy AC. The Role of Environmental Contamination in the Transmission of Nosocomial Pathogens and Healthcare-Associated Infections. Curr Infect Dis Rep. 2018 Apr 27;20(6):12. doi: 10.1007/s11908-018-0620-2. PMID: 29704133.
2. Guest JF, Keating T, Gould D, Wigglesworth N. Modelling the annual NHS costs and outcomes attributable to healthcare-associated infections in England. BMJ Open. 2020 Jan 22;10(1):e033367. doi: 10.1136/bmjopen-2019-033367. PMID: 31974088; PMCID: PMC7045184.
3. Kiernan MA, Garvey MI, Norville P, Otter JA, Weber DJ. Is detergent-only cleaning paired with chlorine disinfection the best approach for cleaning? J Hosp Infect. 2024 Jun;148:58-61. doi: 10.1016/j.jhin.2024.03.018. Epub 2024 Apr 20. PMID: 38649119.
4. Garvey MI, Offorbuzor F, Wilkinson MAC, Kiernan M, Holden E. Chlorine in cleaning - are we concentrating enough? J Hosp Infect. 2025 Jan;155:37-39. doi: 10.1016/j.jhin.2024.09.015. Epub 2024 Oct 5. PMID: 39369992.
5. Westerway SC, Basseal JM, Abramowicz J, Moran C; WFUMB Safety Committee. Recommendations for the Cleaning of Endocavity Ultrasound Transducers Between Patients. Ultrasound Med Biol. 2024 Jun;50(6):775-778. doi: 10.1016/j.ultrasmedbio.2024.02.011. Epub 2024 Mar 14. PMID: 38485533.
6. Sansom SE, Gussin GM, Schoeny M, Singh RD, Adil H, Bell P, Benson EC, Bittencourt CE, Black S, Del Mar Villanueva Guzman M, Froilan MC, Fukuda C, Barsegyan K, Gough E, Lyman M, Makhija J, Marron S, Mikhail L, Noble-Wang J, Pacilli M, Pedroza R, Saavedra R, Sexton DJ, Shimabukuro J, Thotapalli L, Zahn M, Huang SS, Hayden MK. Rapid Environmental Contamination With Candida auris and Multidrug-Resistant Bacterial Pathogens Near Colonized Patients. Clin Infect Dis. 2024 May 15;78(5):1276-1284. doi: 10.1093/cid/ciad752. PMID: 38059527; PMCID: PMC11093678
7. Ledwoch K, Vickery K, Maillard JY. Dry surface biofilms: what you need to know. Br J Hosp Med (Lond). 2022 Aug 2;83(8):1-3. doi: 10.12968/hmed.2022.0274. Epub 2022 Aug 18. PMID: 36066299.
8. Norville P, Dangleben S, Hardy S. Biofilms and Antimicrobial Resistance in Healthcare: Evaluating Chlorine Dioxide as a Candidate to Protect Patient Safety. J Hosp Infect. 2025 May 22:S0195-6701(25)00137-9. doi: 10.1016/j.jhin.2025.04.034. Epub ahead of print. PMID: 40412486